


UKHSA says that Infection-Acquired N-Antibodies are Lower in the Jabbed

Is this a big deal? It might be.
Thanks go to Alex Berenson, banned from Twitter, for bringing this information to light.
Alex thinks it is a big deal:
Take it from a little place I call the British government. Which admitted today, in its newest vaccine surveillance report, that:
“N antibody levels appear to be lower in people who acquire infection following two doses of vaccination.” (Page 23)
What’s this mean? Several things, all bad. We know the vaccines do not stop infection or transmission of the virus (in fact, the report shows elsewhere that vaccinated adults are now being infected at much HIGHER rates than the unvaccinated).
What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus. Specifically, vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people.
This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably).
It also means the virus is likely to select for mutations that go in exactly that direction, because those will essentially give it an enormous vulnerable population to infect. And it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.
Aside from that, everything is fine.
Alex might be right about these things. From the paucity of the information provided from UKHSA Report 42, it's not immediately obvious, but it's certainly concerning.
So, as usual, in order to try to get a clearer picture of what this might mean, I go to the source. The seroprevalence data comes from blood donors and they measure levels of S (spike) antibodies and N (nucleocapsid) antibodies.
The results presented here are based on testing samples with Roche nucleoprotein (N) and Roche spike (S) antibody assays. Nucleoprotein (Roche N) assays only detect post-infection antibodies, whereas spike (Roche S) assays will detect both post-infection antibodies and vaccine-induced antibodies. Thus, changes in seropositivity for the Roche N assay reflect the effect of natural infection. Increases in seropositivity as measured by S antibody reflect both infection and vaccination.
That seems to be fairly clear. Level of N-antibodies exclusively record exposure to natural infection whereas S antibody levels record both natural exposure to the virus and immunisation and apparently, it's impossible to discriminate which is which. So the presence of N-type antibodies is our only reliable guide to exposure to the wild virus. What we don't know is what constitutes an 'infection', whether the presence (or not) of antibodies is a reliable guide to an actual, symptomatic infection whereby the person infected becomes a potential transmitter because of the presence of an actively replicating virus coupled with a sufficiently high viral load present in the nasal cavities. With high viral load, double-jabbed pre or even asymptomatic superspreaders of delta now being a thing, the picture gets complicated. Here is what the report authors say about national prevalence:
Overall population weighted (by age group, sex and NHS region) antibody prevalence among blood donors aged 17 years and older in England was 18.7% (95% CI 17.7% to 19.8%) using the Roche N assay and 98.0% (95% CI 97.7% to 98.3%) using the Roche S assay for the period 16 August to 10 October (weeks 33 to 40 2021). 1,334 out of 7,384 were Roche N positive and 14,815 out of 15,081 samples were Roche S positive. This compares with 14.9% (95% CI 14.1% to 15.8%) Roche N seropositivity and 92.3% (95% CI 91.9% to 92.7%) Roche S seropositivity for the period of 24 May to 13 August 2021 (weeks 21 to 32 2021).
Here are two of the graphs for prevalence:
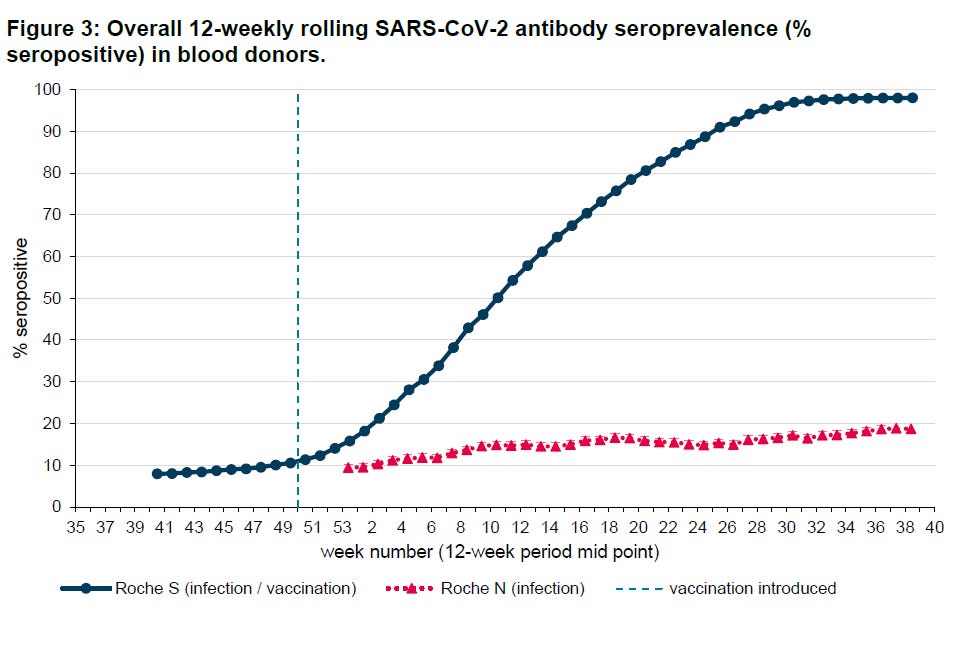

What is immediately clear is that the sharp rise in spike antibodies is almost certainly related to the vaccine rollout beginning in December 2020. The rise in N-Abs is much more gradual and is probably a reflection of gradually increasing prevalence, especially in the younger age groups, who are far less likely to suffer from noticeable symptomatic infections, but may nevertheless contract a very mild form of the virus, enough for their immune systems to generate antibodies against the virus shell. This suggests that the prevalence of the SARS-CoV-2 virus has been increasing, but not at an alarming rate, although there has been a fairly sustained increase in natural infections in people under 40 since about week 23. Here is what the authors have to say about the Roche antibody level serum tests in blood donors:
Roche S seropositivity in blood donors has plateaued and is now over 96% across all age groups. Seropositivity estimates for S antibody in blood donors are likely to be higher than would be expected in the general population and this probably reflects the fact that donors are more likely to be vaccinated. Seropositivity estimates for N antibody will underestimate the proportion of the population previously infected due to (i) blood donors are potentially less likely to be exposed to natural infection than age matched individuals in the general population (ii) waning of the N antibody response over time and (iii) recent observations from UK Health Security Agency (UKHSA) surveillance data that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.
Vaccination has made an important contribution to the overall Roche S increases observed since the roll out of the vaccination programme, initially amongst individuals aged 50 years and above who were prioritised for vaccination as part of the phase 1 programme and more recently in younger adults as part of phase 2 of the vaccination programme.
They suggest that N antibody seropositivity is probably an underestimate because:
(i) blood donors are potentially less likely to be exposed to natural infection than age matched individuals in the general population
(ii) waning of the N antibody response over time
(iii) recent observations from UK Health Security Agency (UKHSA) surveillance data that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.
I can't think why (i) might be an issue. With regards to (ii), antibody levels do definitely wane over time after exposure so this might mean that the shape of the curves above is correct, but they should be shifted up a few percent. But (iii) is a bit of a concern. It seems to suggest that with so many now double-jabbed, exposure to the wild virus is eliciting a more muted N-antibody response in those who have been double-jabbed (the majority of adults) compared to those who have resisted the government's extreme coercion tactics thus far. As N antibody levels are a measure of natural adaptive immunity following exposure to the whole live virus, this might present a serious concern. Will Jones at the Daily Sceptic thinks it could be evidence of Original Antigenic Sin, which I've discussed previously.
A further thing revealed for the first time in this week’s surveillance report is that the vaccines may actually hobble the body’s ability to develop the strongest immunity once infected. As noted by Alex Berenson, the report mentions (in passing) that “recent observations from UK Health Security Agency (UKHSA) surveillance data” show that “N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination”.
There is no elaboration on this, but on the face of it it is a startling admission. It is basically saying that a certain kind of antibody which is not produced by the vaccines but is usually produced by infection (and hence is used by PHE/UKHSA to identify those with antibodies-from-infection) is not produced so well by those who are infected post-vaccination. Insofar as this is true it means the vaccines may actually prevent the immune system from developing the strongest form of protection against reinfection. This phenomenon of the immune system being in some way hobbled by the way it first encounters a pathogen is well-known and is referred to as original antigenic sin.
It might be OAS, but I understood that to be the inability of the immune system to respond effectively to a new variant. So, in the case of the S-directed antibody response elicited by the vaccines, when the vaccinee is exposed to a virus with a significantly changed spike protein, the S-immune response 'remembered' by the trained immune system, will not be sufficient to neutralise the new spike antigen, hence the viral variant will be able to 'escape' vaccine immunity. What we seem to have with the nucleocapsid protein immune response - unique to natural infection - is that it is being diminished somehow because of vaccination. If that's the case, it's not good, not good at all. Why? Because mutated spike variants of the SARS-CoV-2 virus undermine the vaccine immune response (based on obsolete spike versions), but in addition to this, the broad spectrum natural immune response (which is much less affected by mutations in the spike) is also being compromised, which means that double and triple-jabbed people may be in for a very bumpy ride if they come into contact with increasingly more altered spike versions of the SARS-CoV-2 virus.
The importance of the nucleocapsid immune response is outlined below:

The accompanying text explains:
If we group vaccine antibody responses against natural infections, then we see a clear difference (Figure 2).
The data indicates a greater than 2 log increase in nucleocapsid IgG antibody signal after natural infection (median log2 MFI = 8.45) compared to pre-exposure or post-vaccination antibody levels (median log2 MFI = 6.38 and 6.36, respectively).
The following graph shows quite clearly that whereas natural infection elicits both S and N antibodies, vaccination only stimulates S-antibodies and indeed, the J&J vaccine appears to diminish the production of N-type antibodies.

This is further exemplified here:

Figure 3. Antibody signatures against full length SARS-CoV-2 proteins and subunit peptides following vaccination or natural infection. Each participant's pre-vaccine or infection value was subtracted from their post value for each protein or peptide. Cohort values were averaged. Each row indicates a unique peptide or protein. The greater the difference, the more red the color. Blue indicates a decline in antibody binding after the immune event. Values are on Log2 scale. Chart is interactive, use the filter at the top to select specific proteins or peptides to view.
Note that the vaccines, after injection, tend to produce a decline in antibody binding to the nucleocapsid region.
Nucleocapsid is a protein involved in genome packaging and viral assembly. It is not found on the surface of SARS-CoV-2.
S, however, is found on the virus surface, which is the reason it is the dominant immune target after infection.
Due to the greater immune pressure it receives, S protein mutates more rapidly than nucleocapsid. When variants are discussed, the implied variation is in the S protein.
The reduced immune pressure on nucleocapsid helps conserve its sequence and structure, which could mean nucleocapsid antibodies retain effectiveness against emerging SARS-CoV-2 variants.
This explains why it is vitally important to preserve N-antibody response and why infection acquired immunity is more robust than narrow spectrum spike-directed vaccine immunity.