


The British Heartless Foundation Is Putting Children And Young Adults At Risk By Peddling Misinformation And Covering Up Research Data

Here is what Andrew Bridgen had to say about the BHF, in his recent address to Parliament (well, mostly to an empty House, it must be said, because the ‘Right Honourable’ cockroaches couldn’t be arsed to turn up but the world got the message loud and clear):
It has been brought to my attention by a whistleblower from a very reliable source that one of these institutions is covering up clear data that reveals that the mRNA vaccine increased inflammation of the heart arteries.
"They are covering this up in fear that they may lose funding from the pharmaceutical industry.
"The leader of that cardiology research department has a prominent leadership role with the British Heart Foundation and I am very disappointed to say that he has sent out non-disclosure agreements to his research team to ensure that this important data never sees the light of day.
"This is an absolute disgrace. Systemic failure in an over-medicated population also contributes to huge waste of British taxpayers' money and is an increasing strain on the NHS.
This is an explosive claim. Either Bridgen’s whistleblower is not as reliable as he claims or Bridgen is simply lying. Neither of those options look very likely to me. Bridgen is standing almost alone in Parliament by calling into question the safety of the Covid vaccines and calling for them to be withdrawn. He must know the massive forces he is up against and so it seems highly unlikely that he would peddle false or unverified information. He has absolutely nothing to gain from opposing the mainstream ‘safe and effective’ vaccines narrative, but much to lose, I would imagine. Accusing a major health charity of a cover up in Parliament, in front of the world’s cameras, is not something he would do lightly.
I took the time to look at what the BHF were saying about vaccine safety, in particular the risk of myocarditis, and it’s the usual ‘safe and effective’, ‘very rare side effects’, etc. guff:
Does the Covid-19 vaccine cause myocarditis (heart inflammation)?
There have been rare cases of myocarditis (inflammation of the heart muscle) following the Moderna and (even more rarely) Pfizer vaccines in the UK. Myocarditis has also been listed as a rare possible side effect of the Novavax vaccine, after a very small number of cases were reported during clinical trials.
Reports of myocarditis following any Covid-19 vaccine remain rare, and the people who have had this this have usually experienced a mild illness. Those affected have usually quickly felt better with rest and simple treatments.
Research suggests that overall, myocarditis is no more likely to be triggered by a Covid vaccine by than any other vaccine. It's also worth noting that Covid-19 itself is much more likely to cause myocarditis than the vaccine is, and people who are vaccinated have a much lower risk of getting other serious complications caused by Covid-19.
What is the risk of getting myocarditis or pericarditis after the vaccine?
The risk of getting myocarditis or pericarditis after the vaccine is very low.
According to the MHRA's Yellow Card reporting summary, even in the highest-risk age group (18-29), there were just 29 reports of suspected myocarditis or pericarditis for every million second doses of the Pfizer vaccine given in the UK up until 23 November 2022. The risk is even lower following a monovalent Pfizer booster, with just 17 reports per million people in this age group. In other age groups the risk is even lower.
For Moderna, there were 70 cases of suspected myocarditis or pericarditis for every million second doses given in the UK, in this age group. As with the Pfizer vaccine, the risk is much lower after a booster, with just 20 reports per million monovalent Moderna boosters given (up until 23 November 2022). In other age groups the risk is even lower.
They claim to get these figures from the MHRA Yellow Card reporting system, but I’m almost certain that they are wrong and that they vastly underestimate the risk of vaccine-induced myo-pericarditis in young adults and they greatly overestimate the risk of the same condition as a result of infection.
Here is what the BHF say about the risk of myo-pericarditis in children:
Are children and young people at higher risk of heart inflammation from the vaccine?
Cases of heart inflammation (myocarditis or pericarditis) after the vaccine in children and young people are rare.
In the UK up to 23 November 2022, there were 83 cases of myocarditis or pericarditis reported in those under 18 following the vaccine. This is an average rate of 11 cases per million doses. Pfizer is the only vaccine recommended for under-18s).
Overall the rate is lower in children than in adults aged 18-39. There have been no reports of suspected myocarditis or pericarditis following booster doses in under 18s.
The independent Medicines and Healthcare products Regulatory Agency (MHRA) has reviewed all the evidence and confirmed the Pfizer vaccine is safe and effective for children aged 5 and over. This followed an extensive review of the safety, quality and effectiveness of the vaccine in this age group. [Is this some kind of joke?]
As a precaution, the interval between doses is longer for children than for adults, in order to reduce the small risk of developing myocarditis linked to the vaccine. As well as this, if a child (who is not in an at-risk group) gets Covid after their first vaccine dose they should wait 12 weeks from their positive Covid-19 test to have their second jab. This is also to reduce the small risk of developing myocarditis linked to the vaccine.
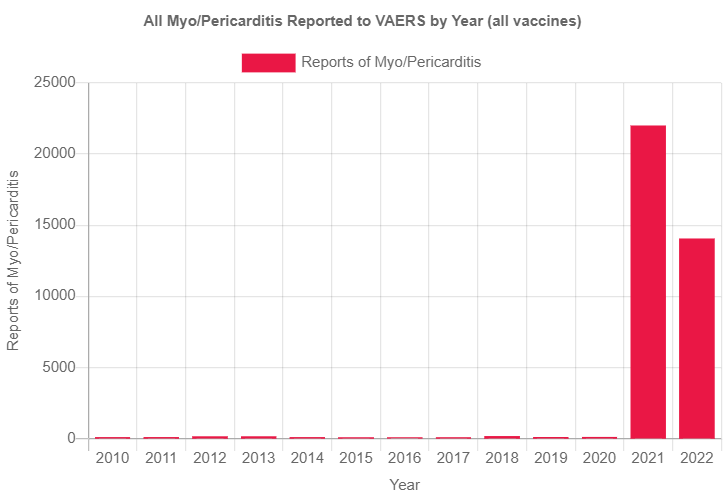
Let’s examine these claims in bold shall we. The BHF rely exclusively, it would seem, upon data from the UK MHRA yellow Card reporting system. Research into myo-pericarditis cases reported after vaccination in other countries tells a very different story. For instance, their claim that “myocarditis is no more likely to be triggered by a Covid vaccine by than any other vaccine”. Yeah? Really? Here’s what the US VAERS data reveals re, ‘flu and all vaccines vs. Covid vaccines:

By not reproducing these graphs in its report and by claiming what it does, I suggest that the British Heartless Foundation is not just guilty of peddling misinformation but of blatantly lying on an epic scale. A Thai study confirmed that rates of myo-pericarditis in younger age groups following Pfizer mRNA vaccination were not just extraordinarily high, but way above that experienced due to other vaccines:
Historically, post-vaccination myocarditis has been reported as a rare adverse event after vaccinations, especially smallpox [4], influenza, and hepatitis B vaccination, among others. In the general population, myocarditis is diagnosed in approximately 10–20 individuals per 100,000 per year [6], and occurs more commonly and at younger ages in males than females [7]. The highest reported incidence of myocarditis from vaccination occurred after a second dose of mRNA COVID-19 vaccine, and mostly among young men [8,9,10]. Most of these cases developed symptoms within the first week, typically 2–4 days post-vaccination. The prognosis for myocarditis patients varies according to etiology [11]. In the pre-COVID-19 era (1990–2018), among 620,195 reports filed in the Vaccine Adverse Event Reporting System (VAERS), 0.1% were attributable to myopericarditis.
So what rate of myo-pericarditis did the Thai study find in adolescents aged 13-18 post Pfizer vaccinations? Well, they sampled 301 people before and after vaccination and SEVEN (all males) suffered from myo-pericarditis, which the authors described as ‘mild’.
The incidence rate of myocarditis/pericarditis after mRNA COVID-19 vaccine was reported to be as low as 12.6 cases per million second dose mRNA vaccines among those aged 12–39 years [8,15]. In contrast, our study found one case of myopericarditis, four cases of subclinical myocarditis, and two cases of pericarditis among 301 participants, and each case had mild symptoms.

One of those 7 required admission to an ICU. All suffered some form of irreparable heart damage because heart muscle does not regenerate. Hardly ‘mild’. Dr Peter McCullough links sudden death to even asymptomatic cases of myocarditis:
Nearly every day there is a report of a young, fit individual, usually a man, who suffers unexplained sudden death now termed “sudden adult death syndrome.” Because COVID-19 vaccination is highly prevalent and linked to the development of heart inflammation and myocarditis, it is a conservative and reasonable conclusion that unless otherwise ruled out, sudden adult death syndrome is a consequence of myocarditis. The differential diagnosis could include other vaccine related serious adverse events including fatal pulmonary embolism, multisystem inflammatory disorder, and vaccine induced thrombocytopenic purpura. Unlike sudden death, most of the other conditions give patients and doctors a chance at making a diagnosis, hospitalization, and treatment. Because half or more of COVID-19 vaccine induced myocarditis is asymptomatic,[i] the first manifestation can be collapse due to an abnormal heart rhythm and unless promptly resuscitated, the pathway to death is rapid and final.

Not mild.
Robert Malone relates the sad case of a 14 year old victim of the Covid jabs:
Two days after her son’s second vaccine dose (which he got a month after his first), he ended up in the hospital after experiencing intense chest pain. He was moved to a room on the acute cardiac floor where he was found to have elevated troponin levels (a key sign of heart damage) and an abnormal electrocardiogram. Every doctor Emily Jo spoke to at the pediatric hospital Children’s Healthcare of Atlanta confirmed her son had vaccine-induced myocarditis.
Given her son’s dire condition, Emily worried Aidan might die or suffer from a catastrophic injury. Thankfully, after four distressful days at the hospital, Aidan troponin levels returned to baseline and he was discharged. However, this didn’t mean he could return to his normal life. Aidan was unable to do physical activity for six months. Sports, hikes, and other forms of exercise were deemed too dangerous for his heart — a typical consequence of myocardial injuries.
“I had no idea how life altering ‘mild’ myocarditis actually is. I have a very hard time with the label ‘mild’ for anything that requires hospitalization and months of inactivity,” Emily Jo said.
Not effing mild! How many times does this have to be said?
Back to the Thai study. 7 cases out of 301 is 2.3%. As a comparison, the BHF is claiming there are 11 cases per million in children under 18. That is 0.001% which is two thousand three hundred times less than what the Thai study found. It’s hard to see that as an innocent mistake and just a modest underestimate. The difference is huge. Other studies have also found high rates of myo-pericarditis in children and young adults which, though not as spectacularly high as the Thai study, are still orders of magnitude in excess of what the British Heartless Foundation claims. Here for instance:
Whatever the true rate of Covid vaccine induced myo-pericarditis in children and young adults is, it is high, much higher than the risk presented by all other vaccines and much higher than the almost zero risk presented by infection in these age groups. The risk/benefit ratio for children and young adults is huge, and this is just for this one condition. Again, I quote Robert Malone:
The risk of death associated with COVID-19 in healthy children is virtually non-existent, as children have significant immunologic advantages relative to the older adult population (> 65 years) which comprises the high risk cohort for COVID-19 (see Omicron has Cracked Open the Overton Window , “We’re never going to learn about how safe this vaccine is unless we start giving it” , and COVID-19 Today).
The risk of death and disease in children has become even more rare with Omicron. Yet even prior to the advent of Omicron, a peer reviewed study clearly demonstrated (using safety data accumulated during past variant circulation) that the genetic COVID-19 vaccines carry a risk/benefit ratio of five deaths in the older, high risk cohort for every one life saved from COVID-19 (and those data did not account for the reporting bias inherent in US deaths due to COVID consequent to inappropriate use of PCR tests). See “Why are we vaccinating children against COVID-19?” (Toxicology Reports, Volume 8, 2021, Pages 1665-1684 ).
RESOLVED, THAT HEALTHY CHILDREN SHALL NOT BE SUBJECT TO FORCED VACCINATION
Negligible clinical risks from SARS-CoV-2 infection exist for healthy children under eighteen.
Long term safety of the current COVID vaccines in children cannot be determined prior to instituting such policies. Without high-powered, reproducible, long term safety data, risks to the long-term health status of children remain too high to support use in healthy children.
Children risk severe, adverse events from receiving the vaccine. Permanent physical damage to the brain, heart, immune and reproductive system associated with SARS-CoV-2 spike protein-based genetic vaccines has been demonstrated in children.
Healthy, unvaccinated children are critical to achieving herd immunity. Natural immunity is proven to tolerate infection, benefiting community protection while there is insufficient data to assess whether COVID-19 vaccines assist herd immunity.
Jessica Rose has an excellent post on the cardiac-related risks posed to children and young adults by these ‘vaccines’.

In summary, the British Heartless Foundation have thrown kids and young adults under the bus and now it looks like they’re deliberately covering up their own damning research data. They’re supposed to save lives, not contribute to deaths in young people by sucking up to their Big Pharma paymasters.
I discovered some time ago that all these health based charities are fronts for organized crime, conning the public out of vast sums of money, which are syphoned back the pharma industry/