


Covid 'Vaccines' - The Unpalatable Truth Plus Why Scientists and Politicians May Have Committed Original Antigenic Sin

This is going to be a long article. There's a lot to cover. I'll try to break it up into bite-sized pieces so it's easier to digest, but even the bite sized pieces are going to be pretty hard to swallow for some who've been suckered into getting jabbed. If you have, what's done is done, but please, whatever you do, don't get a 'booster' jab and don't, if you have an ounce of decency and common sense, allow your kids to get jabbed. In the words of Dr Sucharit Bhakdi:
If you're going for your third, write your will first.
The Vaccinated Superspread Hypothesis (is backed up by data)
We've already seen evidence for virtually unhindered viral transmission amongst double-jabbed health care workers in a hospital in Ho Chi Minh City, Vietnam:
Breakthrough Delta variant infections are associated with high viral loads, prolonged PCR positivity, and low levels of vaccine-induced neutralizing antibodies, explaining the transmission between the vaccinated people.
There's a lot more data coming through though which is suggesting that not only are the double-jabbed just as likely to transmit SARS-CoV-2 as the unjabbed, that not only do they harbour a similar viral load as the unjabbed but they are actually more likely to become infected than the unjabbed. First, let's look at Israel again. This video has been posted on Twitter; a clip from Israeli TV news:
https://twitter.com/Elanders_Voice/status/1441023073562644481
The commentator explains that 90% of cases recorded yesterday were in the double-jabbed and just 10% in the 'unvaccinated'. However, 'unvaccinated' includes partially vaccinated so we don't know for sure what percentage of cases were in the completely unjabbed, but it's probably rather less than 10%, maybe much less. He then goes on to say that the proportion of double-jabbed in Israel is 94%, which means that being double jabbed offers essentially no protection against being infected with delta, now the dominant circulating variant in Israel. What it doesn't tell us is the infection rate in the unjabbed compared to the double or single-jabbed. Supposedly, the 'booster' rollout will address this problem, but it hasn't; infections are still running at record highs, meaning the government is now recommending a fourth jab in a few months time and then a fifth, and sixth, ad nauseum. Absolutely absurd. Essentially, if you get aboard the Covid 'vaccine' conveyor belt, then you are expected to be jabbed every few months as each new variant makes an appearance. You're hooked for life, which with that number of synthetic mRNA injections (coding for a cytotoxic spike protein, which finds its way into most organs of your body including the brain) is likely to be short and increasingly unpleasant.
So, back to the data. Here we have a study titled "Shedding of Infectious SARS-CoV-2 Despite Vaccination" which might equally have been called "Shedding of Infectious SARSCoV2 Because of Vaccination". Why? Because here is what they found:
Low Ct values were detected in vaccinated people regardless of symptoms at the time of testing (Figure 1C). Ct values <25 were detected in 7 of 24 unvaccinated (29%; CI: 13-51%) and 9 of 11 fully vaccinated asymptomatic individuals (82%; CI: 48-97%), and 158 of 232 unvaccinated (68%, CI: 62- 74%) and 156 of 225 fully vaccinated (69%; CI: 63-75%) symptomatic individuals. Time from symptom onset to testing did not vary by vaccination status (p=0.40; Supplemental Figure 2). Infectious virus was detected in the sole specimen tested from an asymptomatic fully vaccinated individual. Although few asymptomatic individuals were sampled, these results indicate that even asymptomatic, fully vaccinated people might shed infectious virus.
Only 29% of unjabbed asymptomatic carriers were highly infectious (Ct<25). A massive 82% of double-jabbed asymptomatic carriers, on the other hand, were similarly highly infectious. This implies that being jabbed makes you a highly infectious asymptomatic superspreader. In those with symptoms, 68% of unjabbed were infectious vs. 69% of those double-jabbed, so no real difference in the symptomatic spreaders.
El Gato Malo's superspread hypothesis is looking more likely according to the data:
the current surge in covid deaths is caused by the vaccinated.
the covid vaccines are extremely leaky and may well accelerate contracting and carrying covid.
they allow for very high viral loads to go unnoticed and generate a new and severe asymptomatic spread vector to where none existed before.
the high viral loads lead to greater contagion. they may lead to greater severity (but this data is iffy and contested)
vaccine campaigns cause superspread events because vaccination leads to a 2 week window of 40-100% more covid risk that then gets counted as “unvaccinated” because the definitions are bad.
this combination makes those vaccinated with one dose or more into superspread bombs.
If you're still not convinced, we have more very recent data from the UK. According to The Daily Sceptic and according to PHE's own data:
None of this concept-policing does anything to alter the facts, however. In recent weeks reported infection rates have been higher in the double vaccinated than in the unvaccinated for the over-40s. That means that, for this period, (unadjusted) vaccine effectiveness is negative in those age groups.
It shows that in the two weeks since my article the vaccine effectiveness has dropped further, with unadjusted vaccine effectiveness in the over-40s now hitting as low as minus-53% among people in their 60s. This means that, on this data for this age group, the double vaccinated experienced a 53% higher reported infection rate than the unvaccinated in the past month. And that’s a fact.
So, it now looks like those people who were jabbed early on (people in their 60s) actually have an increased risk of being infected compared to those who are not jabbed and reliant upon their own natural immunity. This appears to confirm what Geert Vanden Bossche was warning about as early as March this year when he indicated the possibility that immunising people against a narrow part of the virus (which is proving to be highly mutable) might make those immunised more vulnerable when a new variant becomes dominant because the now largely ineffective vaccinated immune response against the new variant might nonetheless suppress the innate immune response. This is the phenomenon known as original antigenic sin and I was warning people about it some time ago on Twitter:
https://twitter.com/JaneDryden4/status/1374392565999357955
https://twitter.com/JaneDryden4/status/1382811297461452801
https://twitter.com/JaneDryden4/status/1392059981244030981
This is what the experts have to say:
The basis of "original antigenic sin" requires immunological memory, and our immune system ability to autocorrect. In the context of viral infections, it is expected that if we are exposed to a native strain of a pathogen, we should be able to mount a secondary immune response on subsequent exposure to the same pathogen. "Original antigenic sin" will not contradict this well-established immunological process, as long as the subsequent infectious antigen is identical to the original one. But "original antigenic sin" implies that when the epitope varies slightly, then the immune system relies on memory of the earlier infection, rather than mount another primary or secondary response to the new epitope which would allow faster and stronger responses. The result is that the immunological response may be inadequate against the new strain, because the immune system does not adapt and instead relies on its memory to mount a response. In the case of vaccines, if we only immunize to a single strain or epitope, and if that strain/epitope changes over time, then the immune system is unable to mount an accurate secondary response. In addition, depending of the first viral exposure the secondary immune response can result in an antibody-dependent enhancement of the disease or at the opposite, it could induce anergy. Both of them triggering loss of pathogen control and inducing aberrant clinical consequences.
Doesn't sound good does it? In the case of the broad spectrum infection acquired immunity to Covid, original antigenic sin would appear not to be an issue because not only does our immune system remember the whole virus (not just a single spike protein), it is also remarkably good at 'guessing' how the virus will mutate in future. In the case of a vaccine-induced narrow spectrum immune response (to the spike region), this looks like it could be a potential problem and now the data is pointing in that direction with regard to delta infections.
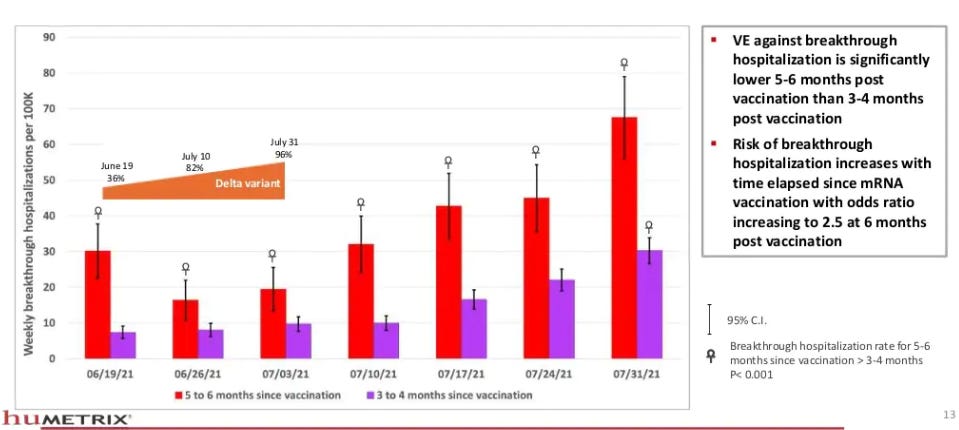
Finally, here is another study of vaccine effectiveness of the mRNA 'vaccines' in 5.6 million Americans aged over 65. The key findings are that since delta appeared, vaccine effectivness has waned considerably, more so in those jabbed early on.


How Effective Are the Vaccines at Preventing Covid Hospitalisations and Deaths?
Remember, this is the key metric by which governments originally sold us the jabs. They would supposedly stop the old and the vulnerable from getting sick and dying in such great numbers, so that when this key cohort was fully jabbed we could rejoice and celebrate the return of our freedoms according to Wanksock. That didn't last long did it? Mission creep turned into an express train. So how are the old and the vulnerable, who got their first jabs six or more months ago, actually doing? Great, according to the ONS:
Some deaths are expected in vaccinated individuals as the number of people who are vaccinated is high and no vaccine is 100% effective. Between 2 January and 2 July 2021, there were 640 deaths involving COVID-19 in people who had received both vaccine doses, which is 1.2% of all deaths involving COVID-19 in that period (51,281 deaths). There were 458 deaths involving COVID-19 in people who received their second dose at least 21 days before the date of death. Deaths involving COVID-19 accounted for 0.8% of all deaths in this group, compared with 37.4% in unvaccinated individuals.
OMG, the unjabbed are dropping like flies compared to the double-jabbed! But the Daily Sceptic exposes the scam:
The ONS has published a new study on Covid deaths which purports to show how few vaccinated people die of Covid. Here’s how the Telegraph reported the headline claim: “Only 59 fully vaccinated people without serious health conditions died from COVID-19 out of more than 50,000 deaths in England this year, new figures from the Office for National Statistics (ONS) show.”
These statistics appear remarkable – until you realise what they’ve done. Although the data is presented as “this year” in fact the cut-off date is July 2nd. That is significant because it is just before the Delta surge got going. This means the data all comes from the Alpha surge, when almost no-one was vaccinated and tens of thousands of Covid deaths were reported, and from the quiet spring and early summer when many were vaccinated but almost no-one died (see chart below).
Comparing the number of deaths in the vaccinated and unvaccinated over this period and presenting it as a percentage is meaningless and to imply it tells us anything about the effectiveness of the vaccines is misleading.
What we need to know is how many jabbed people are dying with the current delta surge. DS provides the answer, using PHE data:
The important question is what the death rates were by vaccination status during the Delta surge, not prior to it.
Public Health England published a report last week which gave us this data for the period of August 9th to September 5th. Here is the table of deaths broken down by vaccination status and age.
This shows that of 2,381 deaths in this period, 1,659 or 69.7%, more than two thirds, were in the double vaccinated. Six hundred deaths or 25.2% were in the unvaccinated. This is very different to the ONS statistics as quoted in the press that 99% of deaths were in those not double vaccinated. Yet no major media outlet compared or contrasted the ONS data with the PHE data released just days ago and asked why there was such a gaping discrepancy.
In the over-50s, the PHE report showed that 1,621 of 2,222 deaths or 73% were in the double vaccinated compared to 499 or 22.5% in the unvaccinated. Once you take into account the proportions of the over-50s vaccinated and unvaccinated this works out at a vaccine effectiveness against death of 68.1% – respectable, but a far cry from the kind of claims being made by the ONS and parroted by the media.
Clearly, with the arrival of delta, the 'vaccines' are not nearly as effective in preventing deaths as was originally claimed and it looks like as time goes on, their effectiveness in preventing infection, serious disease and death is waning considerably.
El Gato Malo has been looking at the deaths and hosptalisations data in US states and detects a clear seasonal signal, varying with latitude, as expected for a seasonal disease. However:
But most worrying is that despite vaccination and despite much more real herd immunity from disease recovery AND a milder variant that, while a bit more contagious, is ~2/3 less lethal, we’re seeing higher cases, deaths, and hospitalizations.
Something is clearly very wrong.
The south and west are dropping in line with seasonal expectation, but the northeast and midwest are rising and are at worse levels than last year by 5X in the NE (most vaccinated part of US) and 2.7X in the MW. testing is about 2X this time last year, so this adjusts down to 2.5X and 1.35X respectively.
And overall hospitalizations are up, not down vs year ago and so are deaths, both by wide margins. (2.5X and 2.7X respectively)
This is not at ALL what one would expect if vaccines were working to stop deaths and hospitalizations (as they seem to be in UK, albeit at closer to 50% VE than the 90’s promised) and with a much lower CFR variant (delta) now predominant. and no, low delta CFR does not look to be a function of vaccines.
Summary So Far
Since the appearance of the delta variant and its dominance in recorded cases:
/ Cases have increased
/ Those double-jabbed have as much virus in their nose and throat as unjabbed people
/ Delta spreads very easily between double-jabbed individuals - the 'vaccines' are having virtually no effect on reducing transmission
/ The double-jabbed appear to be asymptomatic/presymptomatic superspreaders
/ It is looking like those people double-jabbed early on are now more likely to become infected with delta than the unjabbed
/ Ominously, it's looking like highly jabbed populations are experiencing an increase in Covid deaths and hospitalisations as 'vaccine' effectiveness wanes and the jabbed become superspreaders
It Gets Worse - The Jabbed Are Dying in Disproportionate Numbers
The ONS appear to have slipped up again and inadvertently released data which shows the 'vaccinated' are dying in disproportionate numbers from all causes compared to those unjabbed. It's the same data they publicly aired to supposedly 'prove' that the 'vaccines' were effective at preventing deaths, ending July 2nd, which the Daily Sceptic pulled to pieces above. The Expose writes:
This means the unvaccinated account for just 30.3% of deaths, the partly vaccinated account for 37.6% of deaths, and the fully vaccinated account for 32% of deaths due to all causes excluding Covid-19 during the first six months of 2021. Therefore, people who had received a Covid-19 vaccine account for 69.7% of deaths due to all causes excluding Covid-19, with a total of 145,968 people having died.
At first glance you could argue that this would be expected due to the majority of the population allegedly having received a Covid-19 vaccine. However, these deaths did not all occur once the majority of the population had been vaccinated.
60% of deaths due to all causes between January 2nd 2021 and July 2nd 2021 occurred during the first three months, the majority of these occurring in January, followed by February, and then March.
By the end of these three months 47.6% of the population had received a single dose of a Covid-19 vaccine, and just 7.4% of the population had received a second dose of a Covid-19 vaccine.
Even by July 2nd 2021 just 67.6% of the population had received a single dose of a Covid-19 vaccine, whilst 50.2% of the population had received a second dose of a Covid-19 vaccine.
We cannot say for sure that the unjabbed are dying in disproportionate numbers because of the limitations of the ONS data, but it very much looks that way from the data they have supplied.
It would be helpful to have more data on deaths by vaccination status, such as the date of occurrence, in order to come to a firm conclusion.
However, what we do know is that the majority of deaths due to all causes occurred during the first three months of 2021 when the number of people to have received a single dose of a Covid-19 vaccine ranged from 2% to 47.6% and the number of people to have received a second dose ranged from 0% to just 7.4%.
Couple the above with data published by Public Health England which shows 72% of Covid-19 deaths due to the Delta Covid-19 variant have been among the vaccinated population since February 1st up to September 12th, and 74% of Covid-19 deaths due to the Delta Covid-19 variant have been among the vaccinated population since August 2nd and September 12th, then it is possible to conclude that the Covid-19 vaccines are not working, and have killed thousands.
Of course, The Expose is a 'conspiracy' site. We know this because it keeps getting banned by Twitter, therefore we can't believe the facts which they publish online, so for completeness let's look at what Queen Mary College London analysts Norman Fenton and Martin Neil have to say on their Probability and Risk blog:
The UK Government's own data does not support the claims made for vaccine effectiveness/safety.
In a previous post we argued that the most reliable long-term measure of Covid-19 vaccine effectiveness/safety is the age adjusted all-cause mortality rate. If, over a reasonably prolonged period, fewer vaccinated people die, from whatever cause, including Covid-19, than unvaccinated people then we could conclude that the benefits of the vaccine outweigh the risks.
The latest Office for National Statistics report on mortality rates by Covid vaccination status provides data on all deaths – Covid related and non-Covid related for the period Jan-July 2021 for the unvaccinated and the different categories of vaccinated ('within 21 days of first dose', '21 days or more after first dose', 'second dose').
We believe there are severe weaknesses and possible errors in the ONS data (see foonote**). But importantly, while it does not provide the raw age categorized data, it does provide "age standardized" mortality rates***. This means the ONS have calculated the overall mortality rate in a way which (they believe) adjusts for the confounding effect of age, and this is ‘baked into’ the mortality rates they have published. However, while they report this age adjusted mortality rate for each of the three separate categories of vaccinated people they do not report it for the combined set of vaccinated people. In our analysis, and in the absence of the actual age stratified data, we compute a population weighted age adjusted all-cause mortality rate by using the ONS’s published population sizes for each of the three categories of vaccinated. This is not ideal because the ONS age adjusted rates are so opaque and are not 'abolute numbers'. However, in the absence of detailed data this should provide a reasonable estimate of what the ONS age adjusted all-cause mortality rate would be for all unvaccinated if they had bothered to report it. We will call this the ‘weighted vaccinated mortality rate’. The data table derived from the ONS data and used to compute this rate is given at the end of this post.
It turns out that, even using this age adjusted mortality rate, the death rate is currently higher among the vaccinated than the unvaccinated.
Because of the limitations and possible errors in the ONS data**, there are many caveats that need to be applied to our crude analysis (including some which are covered in the previous post). But we can conclude that the ONS's own data does not support the claims made for vaccine effectiveness/safety.
So there you have it. A more rigorous analysis of the ONS data, by expert statisticians, confirms that the jabbed are dying at a greater rate from all causes, not just Covid, than are the unjabbed. How on earth could this be you ask? The 'vaccines are supposed to save lives, not expedite our demise. Some of the answers to that question have been staring us in the face for months and I've provided quite a few hints here on my own humble blog.
Covid 'Vaccine' Harms
Sarah Knapton at the Telegraph published an interesting article yesterday, highlighting facts for a change, not opinion or gossip, which most of the MSM has excelled in for 18 months. It's titled, provocatively:
Thousands more people than usual are dying ... but it’s not from Covid
She writes:
While focus remains firmly fixed on Covid-19, a second health crisis is quietly emerging in Britain. Since the beginning of July, there have been thousands of excess deaths that were not caused by coronavirus.
According to health experts, this is highly unusual for the summer. Although excess deaths are expected during the winter months, when cold weather and seasonal infections combine to place pressure on the NHS, summer generally sees a lull.
This year is a worrying outlier.
Whatever can be wrong? Sarah puts it all down to delays in treatment and compromised population immunity due to lockdowns. Without doubt, these must be factors, especially the dirt poor 'health' service now very reluctantly granted grudgingly as a favour to citizens by elitist NHS GPs intent on not seeing patients. Many urgent, life threatening cases are going undiagnosed as a result, but still there is a huge backlog of outpatient appointments at hospitals. However, what our national newspaper science editor fails to reveal is the very analysis above which reveals that the jabbed are dying at a greater rate than the unjabbed. There is a clue in her article though as to what is killing significant numbers of people and, as it happens, this appears to coincide with reported serious adverse reactions to the jabs:
Data from Public Health England (PHE) shows that during that period there were 2,103 extra death registrations with ischemic heart disease, 1,552 with heart failure, as well as an extra 760 deaths with cerebrovascular diseases such as stroke and aneurysm and 3,915 with other circulatory diseases.
Nothing like investigative science journalism which is short on investigation and leaves out relevant science, eh? Wouldn't want to upset Pol Pot Belly and Rabid Jabid though. So must tread carefully.
At the recent FDA advisory group meeting where the board voted 16-2 not to roll out mRNA booster jabs to the general populace, Steve Kirsch, Executive Director of the Covid-19 Early Treatment Fund, made a remarkable claim:
“I’m going to focus my remarks today on the elephant in the room that nobody likes to talk about, that the vaccines kill more than they save."
“We were led to believe that the vaccines were perfectly safe but this is simply not true, for example there are four times as many heart attacks in the treatment group in the Pfizer 6 month file report, that wasn’t just bad luck. VAERS shows heart attacks happen 71 times more often following these vaccines compared to any other vaccine,
“Only the VAERS (Vaccine Adverse Event Reporting System) are statistically significant, but the other numbers are troubling.
“Even if the vaccines have 100% protection, it still means we kill 2 people to save 1 life.
“Four experts did analysis using completely different non US data sources and all of them came up with approximately the same number of excess vaccine related deaths, about 411 deaths per million doses. That translates into 115,000 people have died (due to the Covid-19 vaccines).
“The real numbers confirm that we kill more than we save. And I would love to look at the Israel ministry of health data on the 90+ year olds where we went from a 94.4% vaccinated group to 82.9% vaccinated in the last 4 months.
“In the most optimistic [case] it means that 50% of the vaccinated people died and 0% of unvaccinated people died. Unless you can explain that to the public you cannot approve the boosters.”
Steve Kirsch, who is also a 'conspiracy theorist', having been banned from Twitter, can be found on Gab. He has recently dug up this devastating paper, appearing in Toxicology Reports. The findings of this study should seriously concern everyone. The Abstract says:
This article examines issues related to COVID-19 inoculations for children. The bulk of the official COVID-19-attributed deaths per capita occur in the elderly with high comorbidities, and the COVID-19 attributed deaths per capita are negligible in children. The bulk of the normalized post-inoculation deaths also occur in the elderly with high comorbidities, while the normalized post-inoculation deaths are small, but not negligible, in children. Clinical trials for these inoculations were very short-term (a few months), had samples not representative of the total population, and for adolescents/children, had poor predictive power because of their small size. Further, the clinical trials did not address changes in biomarkers that could serve as early warning indicators of elevated predisposition to serious diseases. Most importantly, the clinical trials did not address long-term effects that, if serious, would be borne by children/adolescents for potentially decades.
A novel best-case scenario cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreases drastically as age decreases, and the longer-term effects of the inoculations on lower age groups will increase their risk-benefit ratio, perhaps substantially.
Here is a list of the known and potential side effects of the Covid 'vaccines', according to the authors:
We believe that mid-or long-term adverse effects are possible based
on the recent emergence of evidence that would support the probability
of mid-and long-term adverse effects from the COVID-19 inoculants,
such as:
1) The spike protein itself can be a toxin/pathogenic protein:
2) S protein alone can damage vascular endothelial cells (ECs) by
downregulating ACE2 and consequently inhibiting mitochondrial
function [37].
3) it is concluded that ACE2 and endothelial damage is a central part
of SARS-CoV2 pathology and may be induced by the spike protein
alone [38].
4) the spike protein of SARS-CoV-1 (without the rest of the virus)
reduces ACE2 expression, increases angiotensin II levels, exacerbates
lung injury, and triggers cell signaling events that may
promote pulmonary vascular remodeling and Pulmonary Arterial
Hypertension (PAH) as well as possibly other cardiovascular
complications [39].
5) the recombinant S protein alone elicits functional alterations in
cardiac vascular pericytes (PCs) [40]. This was documented as:
6) increased migration
7) reduced ability to support EC network formation on Matrigel
8) secretion of pro-inflammatory molecules typically involved in the
cytokine storm
9) production of pro-apoptotic factors responsible for EC death.
Furthermore, the S protein stimulates the phosphorylation/activation
of the extracellular signal-regulated kinase 1/2 (ERK1/2)
through the CD147 receptor, but not ACE2, in cardiac PCs, the S
protein may elicit vascular cell dysfunction, potentially amplifying,
or perpetuating, the damage caused by the whole coronavirus
[40].
10) “even in the absence of the angiotensin-converting enzyme 2
receptors, the S1 subunit from SARS-CoV-2 spike protein binding
to neutral phospholipid membranes leads to their mechanical
destabilization and permeabilization. A similar cytotoxic effect of
the protein was seen in human lung epithelial cells.” [125].
11) The LNP layer encapsulating the mRNA of the inoculant is highly
inflammatory in both intradermal and intranasal inoculation
[41] and “Polyethylene glycol (PEG) is a cause of anaphylaxis to
the Pfizer/BioNTech mRNA COVID-19 vaccine” [42]. “Humans
are likely developing PEG antibodies because of exposure to
everyday products containing PEG. Therefore, some of the immediate
allergic responses observed with the first shot of
mRNA-LNP vaccines might be related to pre-existing PEG antibodies.
Since these vaccines often require a booster shot,
anti-PEG antibody formation is expected after the first shot. Thus,
the allergic events are likely to increase upon re-vaccination”
[43].
There is also the possibility that the components of the LNP
shell could induce the ASIA Syndrome (autoimmune/
inflammatory syndrome induced by adjuvants), as
shown by studies on post-inoculation thyroid hyperactivity [44]
and post-inoculation subacute thyroiditis [45].
12 The spike protein has been found in the plasma of postinoculation
individuals, implying that it could circulate to, and
impact adversely, any part of the body [46].
13 The spike protein of SARS-CoV-2 crosses the blood-brain barrier
in mice [47], and “the SARS-CoV-2 spike proteins trigger a
pro-inflammatory response on brain endothelial cells that may
contribute to an altered state of BBB function” [48].
14 The spike proteins manufactured in vivo by the present COVID-19
inoculations could potentially "precipitate the onset of autoimmunity
in susceptible subgroups, and potentially exacerbate
autoimmunity in subjects that have pre-existing autoimmune
diseases", based on the finding that anti-SARS-CoV-2 protein
antibodies cross-reacted with 28 of 55 diverse human tissue antigens
[49].
15 “The biodistribution of ChaAdOx1 [Astra Zeneca’s recombinant
adenovirus vaccine candidate against SARS-CoV-2] in mice
confirmed the delivery of vaccine into the brain tissues [50]. The
vaccine may therefore spur the brain cells to produce CoViD spike
proteins that may lead to an immune response against brain cells,
or it may spark a spike protein-induced thrombosis. This may
explain the peculiar incidences of the fatal cerebral venous sinus
thrombosis (CVST) observed with viral vector-based CoViD-19
vaccines” [51,52].
A complementary perspective to explain adenovirus-based
vaccine-induced thrombocytopenia is that “transcription of
wildtype and codon-optimized Spike open reading frames enables
alternative splice events that lead to C-terminal truncated,
soluble Spike protein variants. These soluble Spike variants may
initiate severe side effects when binding to ACE2-expressing
endothelial cells in blood vessels.” [100].
16 A Pfizer Confidential study performed in Japan showed that
"modRNA encoding luciferase formulated in LNP comparable to
BNT162b2′′ injected intramuscularly concentrated in many organs/
tissues in addition to the injection site [53]. The main
organs/sites identified were adrenal glands, liver, spleen, bone
marrow, and ovaries. While damage to any of these organs/sites
could be serious (if real for humans), adverse effects on the
ovaries could be potentially catastrophic for women of childbearing
or pre-childbearing age.
Talking of the effect of spike proteins on the endothelial lining of the blood vessels, the authors state the following:
These effects can occur throughout the body in the short term, as we
are seeing with the VAERS results. They can occur in the mid- and longterm
as well, due to the time required for destructive processes to have
full effect and the administration of further inoculations. For example,
micro-clots resulting from the inoculation that were insufficient to cause
observable symptoms could in effect raise the baseline for thrombotic
disease [92]. Lifestyle activities that contribute to enhanced blood
clotting would have less distance to travel to produce observable
symptoms, and thus the serious effects of clotting would have been
accelerated [59,60]. As an example: the risk of venous thrombosis is
approximately 2- to 4-fold increased after air travel [61]. How much this
rate would increase after the inoculations, where microthrombi have
formed in some recipients, is unknown. These potential baseline-raising
effects could impact the interpretation of the VAERS results, as we show
at the end of Appendix 1.
The authors perform a cost-benefit analysis using the VAERS data, known clinical pathology associated with injection of the 'vaccines' and projections of long and mid term effects and they come to this devastating conclusion:
Thus, our extremely conservative estimate for risk-benefit ratio is about 5/1. In plain English, people in the 65+ demographic are five times as likely to die from the inoculation as from COVID-19 under the most favorable assumptions! This demographic is the most vulnerable to adverse effects from COVID-19. As the age demographics go below about 35 years old, the chances of death from COVID-19 become very small, and when they go below 18, become negligible.
It should be remembered that the deaths from the inoculations shown in VAERS are short-term only (˜six months for those inoculated initially), and for children, extremely short-term (˜one month) [3]. Intermediate and long-term deaths remain to be identified, and are possible from ADE, autoimmune effects, further clotting and vascular diseases, etc., that take time to develop. Thus, the long-term cost-benefit ratio under the best-case scenario could well be on the order of 10/1, 20/1, or more for all the demographics, increasing with decreasing age, and an order-of-magnitude higher under real-world scenarios! In summary, the value of these COVID-19 inoculations is not obvious from a cost-benefit perspective for the most vulnerable age demographic, and is not obvious from any perspective for the least vulnerable age demographic.
Is Now The Winter Of Our Discontent?
It certainly looks like it in the UK. We're looking at soaring energy bills, possible major blackouts, fuel shortages, possibly food shortages, a crisis of health care (all mostly manufactured by the media and by government incompetence/calculated planning), soaring respiratory infections and escalating deaths due to all causes, a government chomping at the bit to introduce more restrictions and lockdowns and justify the introduction of totally useless vaccine passports whose only real purpose is to act as an entry-level digital ID for a globally enforced social credit system allied with digitalised central bank currencies. Then there's the alleged 'climate crisis' (a Guardian style guide invention) which we'll be plugged with ad nauseum in the run up to COP 26 and have our journeys interrupted by paid 'climate protestors' blocking roads (assuming we can fill up the car). Not to put too fine a point on it, some people (maybe a lot of people are not going to make it through this coming hell winter and a large part of the blame for the coming carnage will fall at the feet of our politicians and a craven main stream media who have created the 'crises' which we will be facing. Original sinners, one and all, who most likely have also committed original antigenic sin; thus the last word must go to Geert Vanden Bossche in his recent article, The Last Post:
It’s important to note that a high background level of innate population-level immunity will prevent the virus from wiping out a whole population. Part of this immunological capacity will be eroded as the infectious pressure rises; however, it will subsequently be replaced by robust, naturally acquired immunity when people who became vulnerable recover from the disease. This mechanism enables the host population to keep the virus under control while – in return - providing the virus with a renewable reservoir for asymptomatic transmission (i.e., by virtue of asymptomatically infected people). This is how Sars-CoV-2 could have become endemic.
Let’s now consider the additional impact of human intervention on the Sars-CoV-2 pandemic. Human intervention too may have both detrimental and beneficial effects which may be age-dependent as well and equally evolve over time. More importantly, influences from human intervention will interfere with those caused by the evolutionary dynamics of a natural pandemic. Infection prevention measures may, for example, have a beneficial short-time effect in that they diminish viral transmission and, therefore, reduce morbidity rates in vulnerable people (i.e., primarily in the elderly). In the longer run, however, they may lead to insufficient training of innate immune mechanisms, which would primarily become manifest in those who primarily rely on innate immunity as a first line of immune defense (i.e., children).
There should be no doubt that non-transmission-blocking vaccines (i.e., so-called ‘leaky’ or ‘imperfect’ vaccines) can never ever control a pandemic, even though they may temporarily protect against disease.
Given the globally increasing immune pressure and concomitant infectious viral pressure, genomic epidemiologists have no doubt that this pandemic roller coaster will not stop before it takes us over the cliff into the abyss of complete viral resistance to anti-spike (S) antibodies. That is where all runaway trains of the different ongoing pandemics of highly infectious variants will be coming together and converge into a big whirl where they can no longer be distinguished from one another. The first stages of this evolution is what we now begin to see in countries which have already massively vaccinated their population (e.g., Israel). There is no doubt that other countries like the United Kingdom and the United States will soon go down the same path. Due to increasing resistance to neutralizing anti-S antibodies (Abs), these countries are now even beginning to shift from a primarily beneficial (i.e., less susceptible to severe disease) to a primarily detrimental effect (more susceptible to severe disease) in the vaccinated as compared to the unvaccinated (https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201).
The current situation is highly problematic as ALL segments of the population will dramatically suffer from a situation where anti-S Abs still bind strongly enough to suppress the vaccinee’s innate immune response against non-mutable, highly conserved Coronavirus (CoV) motifs while no longer being able to sufficiently neutralize highly infectious variants. Instead, poor binding affinity of anti-RBD (receptor-binding domain) Abs to Sars-CoV-2 S protein as a result of mutations in the N-terminal domain (NTD) could tip the scale in favor of infection-enhancing Abs and thereby make vaccinees prone to suffering Ab-dependent enhancement (ADE) of Covid-19 disease (1) (Liu et al., 2021; Yahi N et al., 2021).
Viral resistance to these S-specific Abs is a terrifying thought as spike protein is not only required but sufficient for enabling CoV infectiousness and pathogenicity (Belouzard S, 2012; Weiss and Navas-Martin, 2005).
The mass vaccination hype will undoubtedly enter history as the most reckless experiment in the history of medicine. It will be cited as the unequivocal proof of how overuse or misuse of man-made antimicrobials leads to antimicrobial resistance, regardless of whether the antimicrobial is an antibiotic or an antibody administered through passive immunization or elicited via active immunization. Mass vaccination campaigns conducted in the middle of a viral pandemic will, for generations to come, become the most sobering example of the boundaries of human intervention in nature in general and of the boundaries of conventional vaccinology in particular. This irrational experiment will unambiguously highlight the clear-cut limitations of conventional vaccine approaches. It will convincingly illustrate that – unlike natural acute self-limiting infection or disease – ‘modern’ technologies alone do not suffice to develop vaccines that are capable of preventing viral transmission or immune escape.
Summary of 'Vaccine' Harms
/ Huge and unprecedented numbers of serious adverse reactions and deaths compared to other vaccines
/ 'Vaccines' killing more people than saving, potentially killing a lot more people in the medium to long term
/ Well defined set of clinical symptoms associated with adverse reactions and deaths due to 'vaccination'
/ Spike proteins and lipid mRNA envelope causing a lot of the clinical symptoms - microclots a long term risk multiplier.
/ Data showing that the death rate from all causes in the double-jabbed exceeds that of the unjabbed
/ Mass vaccination with leaky vaccines will potentially extend the pandemic and make matters a lot worse
/ Booster jabs will ony exacerbate the situation and quite likely seriously harm many individuals who get them
My advice to those jabbed and unjabbed. Get some Ivermectin in stock and take Vitamin D supplements throughout the dark winter months. Don't let your kids get jabbed. Do not get a booster jab at any price. Let's stay warm, stay healthy and let's hopefully stay together through this very challenging coming winter (not forgetting an extremely challenging coming summer for our friends Down Under).
Update 26th September:
This research article was brought to my attention on Twitter:
Review of data from the three COVID-19 vaccines marketed in the US shows complete lack of a health benefit and even an increase in severe events among vaccine recipients. The proper scientific clinical trial endpoint, “all cause severe morbidity” was created by combining all severe and or life threatening events, both infectious and non-infectious, occurring in the vaccinated and placebo control groups respectively. The data (Table 1) shows there are clearly more severe events in the vaccinated groups. The results are highly statistically significant. The use of a true scientific measure of health as an endpoint for a vaccine trial gives a contrasting result compared to the use of a non-scientific surrogate endpoint of heath, severe infections with COVID-19.